
This article provides a brief overview of the pivotal role of the complement system during the contraction phase of the immune response. It highlights how complement orchestrates the efficient clearance of apoptotic cells, apoptotic bodies, and immune complexes, thereby promoting the resolution of inflammation, preserving self-tolerance, and preventing the development of autoimmune diseases.
The complement system is a vital component of the innate immune system that bridges innate and adaptive immunity through a tightly regulated cascade of plasma proteins. Although it is best known for its role in pathogen recognition, opsonization, and elimination, complement also performs essential regulatory functions during the later stages of an immune response. By facilitating the non-inflammatory clearance of apoptotic cells and immune complexes, the complement system promotes immune response contraction and contributes to the restoration of immune homeostasis.
The contraction phase of the immune response
Once an invading pathogen has been effectively controlled, the adaptive immune response enters a tightly regulated contraction phase that restores immune equilibrium. At this stage, the expanded population of effector T and B lymphocytes is substantially reduced through programmed cell death (apoptosis), while a small pool of antigen-specific memory cells is preserved to provide long-term immune protection. Meanwhile, antigen–antibody complexes generated during the immune response may persist in the circulation and lymphoid tissues. The efficient clearance of these apoptotic cells and immune complexes is essential to prevent persistent inflammation, tissue damage, and the development of autoimmune disorders. The complement system plays a central role in orchestrating these clearance mechanisms, thereby facilitating immune resolution and the restoration of tissue homeostasis.
Recognition of Apoptotic Cells by the Complement System
One of the earliest events during apoptosis is the loss of membrane asymmetry, resulting in the externalization of phosphatidylserine (PS), a phospholipid that is normally confined to the inner leaflet of the plasma membrane in healthy cells. The appearance of phosphatidylserine on the cell surface serves as an important “eat-me” signal, indicating that the cell is destined for removal. Serum proteins, particularly annexin A5, readily bind to the exposed phosphatidylserine and facilitate its recognition by the complement component C1q. As apoptosis progresses, additional characteristic changes occur, including chromatin condensation, nuclear fragmentation, DNA cleavage, and the exposure of nuclear constituents on the cell surface.
C1q can also directly recognize extracellular DNA, along with specific glycoproteins and phospholipids displayed on apoptotic cells. During the later stages of apoptosis, dying cells fragment into membrane-enclosed structures known as apoptotic bodies, which continue to expose phosphatidylserine, DNA, and other molecular signatures associated with cell death. These collectively provide multiple recognition sites for C1q, enabling the complement system to efficiently identify apoptotic cells and their fragments for subsequent clearance by phagocytes.
Complement-Mediated Clearance of Apoptotic Cells
The binding of C1q to apoptotic cells and apoptotic bodies serves as a critical signal for their efficient removal by phagocytic cells. C1q-coated apoptotic material is recognized by C1q receptors (C1qRs) expressed on macrophages and other professional phagocytes, promoting its engulfment and degradation. In addition to functioning as a recognition molecule, C1q can initiate the classical complement pathway, resulting in the deposition of C3b and its cleavage products on the surface of dying cells. These complement fragments act as potent opsonins and are recognized by complement receptor 1 (CR1) on macrophages, further enhancing phagocytosis and ensuring the rapid, non-inflammatory clearance of cellular debris.
Studies in C1q-deficient mice highlight the crucial role of C1q in maintaining immune homeostasis. In the absence of C1q, apoptotic cells are cleared inefficiently, allowing apoptotic bodies and membrane blebs to accumulate and persist within tissues. These uncleared cellular remnants can expose intracellular self-antigens to the immune system, increasing the likelihood of autoantibody production and the initiation of autoimmune responses. Consequently, C1q-deficient mice exhibit elevated levels of autoantibodies, increased mortality, and a greater incidence of glomerulonephritis, an autoimmune disease characterized by inflammation of the kidney glomeruli. Histological examination of their kidneys further reveals the accumulation of apoptotic bodies together with immune complex deposits, highlighting the indispensable role of C1q in preventing autoimmune pathology through the timely clearance of dying cells.
Complement-Mediated Clearance of Immune Complexes
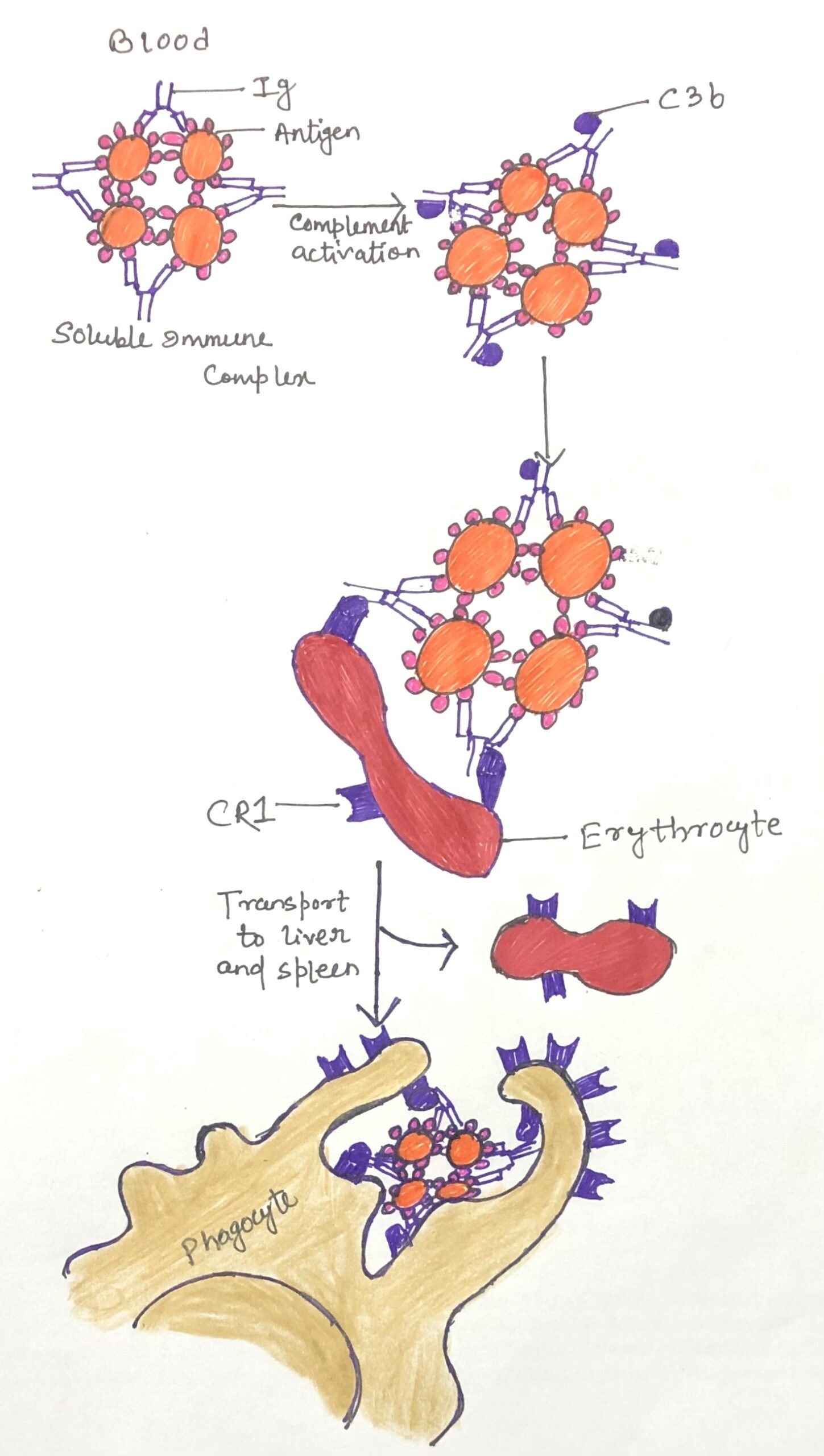
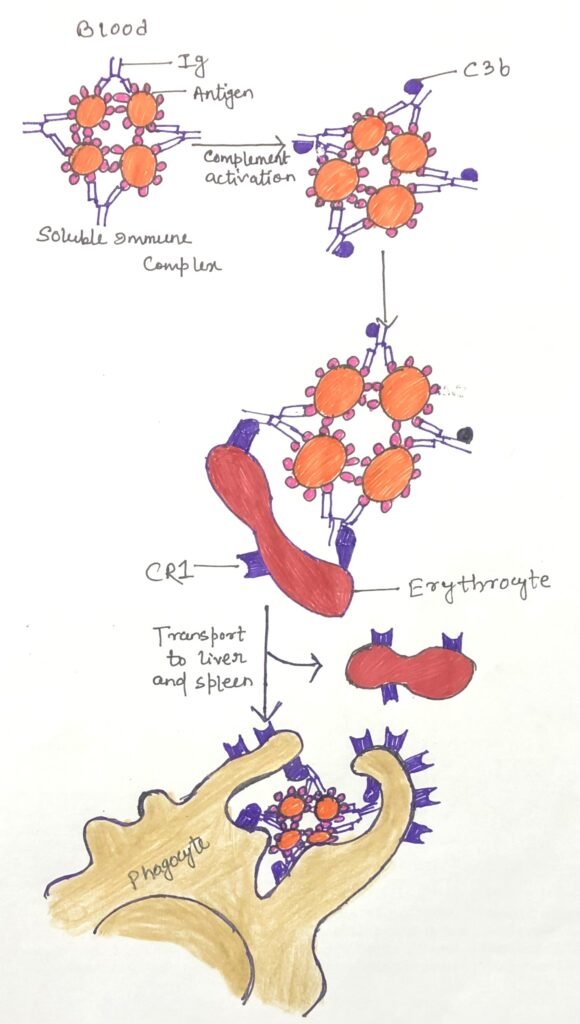
During the contraction phase of an immune response, soluble antigen–antibody complexes that remain in the circulation must be efficiently eliminated to prevent tissue injury and chronic inflammation. The complement system plays a central role in this process by depositing C3b onto immune complexes, thereby opsonizing them for safe removal. These C3b-coated complexes are recognized by complement receptor 1 (CR1/CD35) expressed on erythrocytes (red blood cells). Although individual erythrocytes display relatively few CR1 molecules compared with leukocytes, their overwhelming abundance in the bloodstream makes them the principal carriers of circulating immune complexes. Consequently, nearly 90% of the CR1 present in peripheral blood is found on erythrocytes.
After binding immune complexes, erythrocytes transport them to the liver and spleen, where resident macrophages detach and phagocytose the opsonized complexes without destroying the red blood cells (Figure 1). This highly efficient transport system prevents immune complexes from accumulating in tissues and limits unnecessary complement activation, thereby promoting the resolution of inflammation and preserving immune homeostasis.
The physiological importance of this clearance mechanism is highlighted in systemic lupus erythematosus (SLE), an autoimmune disease characterized by impaired immune-complex disposal. In individuals with SLE, circulating immune complexes are inadequately cleared and instead become deposited within tissues such as the kidneys, skin, joints, and blood vessels. These deposits continuously activate the complement system, triggering persistent inflammation and progressive tissue damage that contribute to the clinical manifestations of the disease.
The C4 Deficiency Paradox in Systemic Lupus Erythematosus (SLE)
An intriguing aspect of SLE is its strong association with deficiencies in the early components of the classical complement pathway, particularly C4. Although complement activation contributes to inflammatory tissue injury in established SLE, individuals with complete C4 deficiency are at a markedly increased risk of developing the disease. This apparent paradox can be explained by the crucial role of C4 in initiating effective opsonization. In the absence of sufficient C4, reduced activation of the classical pathway results in diminished C3b deposition on immune complexes, impairing their recognition and clearance by CR1-bearing erythrocytes and phagocytes. The persistence of these uncleared immune complexes ultimately promotes autoimmunity and sustained inflammatory responses, underscoring the indispensable role of complement in maintaining immune tolerance and facilitating immune response contraction.
Conclusion
Although the complement system is traditionally recognized for its role in host defense against invading pathogens, it is equally indispensable during the contraction phase of the immune response. By recognizing and opsonizing apoptotic cells, apoptotic bodies, and soluble immune complexes, complement facilitates their efficient, non-inflammatory clearance through phagocytic cells and erythrocyte-mediated transport.
These mechanisms prevent the accumulation of cellular debris and immune complexes that could otherwise sustain inflammation or trigger autoimmune reactions. The association of complement deficiencies, particularly involving C1q and C4, with disorders such as systemic lupus erythematosus highlights the critical importance of these clearance pathways in maintaining self-tolerance. Thus, beyond its antimicrobial functions, the complement system serves as a key regulator of immune resolution, ensuring the timely restoration of immune homeostasis and protecting tissues from the harmful consequences of an unresolved immune response.
You may also like:

I, Swagatika Sahu (author of this website), have done my master’s in Biotechnology. I have around fourteen years of experience in writing and believe that writing is a great way to share knowledge. I hope the articles on the website will help users in enhancing their intellect in Biotechnology.