
In this article, I briefly describe type-I hypersensitive reactions and their effects.
Hypersensitivity
Hypersensitivity pertains to the inflammatory reactions within the humoral or cell-mediated branches of the immune system, causing extensive tissue damage or occasionally death. The reactions are immediate or may be delayed type, depending on the symptoms.
P.G.H. Gell and Robin Coombs categorized hypersensitive reactions into four types in 1963. The four types of reactions are named type-I, type-II, type-III, and type-IV hypersensitivity reactions. The type-I, type-II, and type-III hypersensitive reactions are mediated by antibody or antigen-antibody complexes within the humoral branch of the immune system.
Type-IV hypersensitivity is a delayed-type hypersensitivity that occurs within the cell-mediated branch of the immune system. Immediate hypersensitivity includes the symptoms that manifest within minutes or hours after a sensitized recipient encounters an antigen. Type-4 hypersensitivity includes the delayed onset of symptoms after exposure to an antigen, also called delayed-type hypersensitivity.
Type-I Hypersensitive Reaction
The Type I hypersensitive reaction comes under immediate hypersensitivity, which is an allergic reaction. Certain types of antigens, known as allergens, induce type-I hypersensitive reactions. The reaction may be local or systemic and resembles a normal humoral response. It may involve the skin (urticaria and eczema), eyes (conjunctivitis), nasopharynx (rhinitis), bronchopulmonary tissues (asthma), and gastrointestinal tract (gastroenteritis).
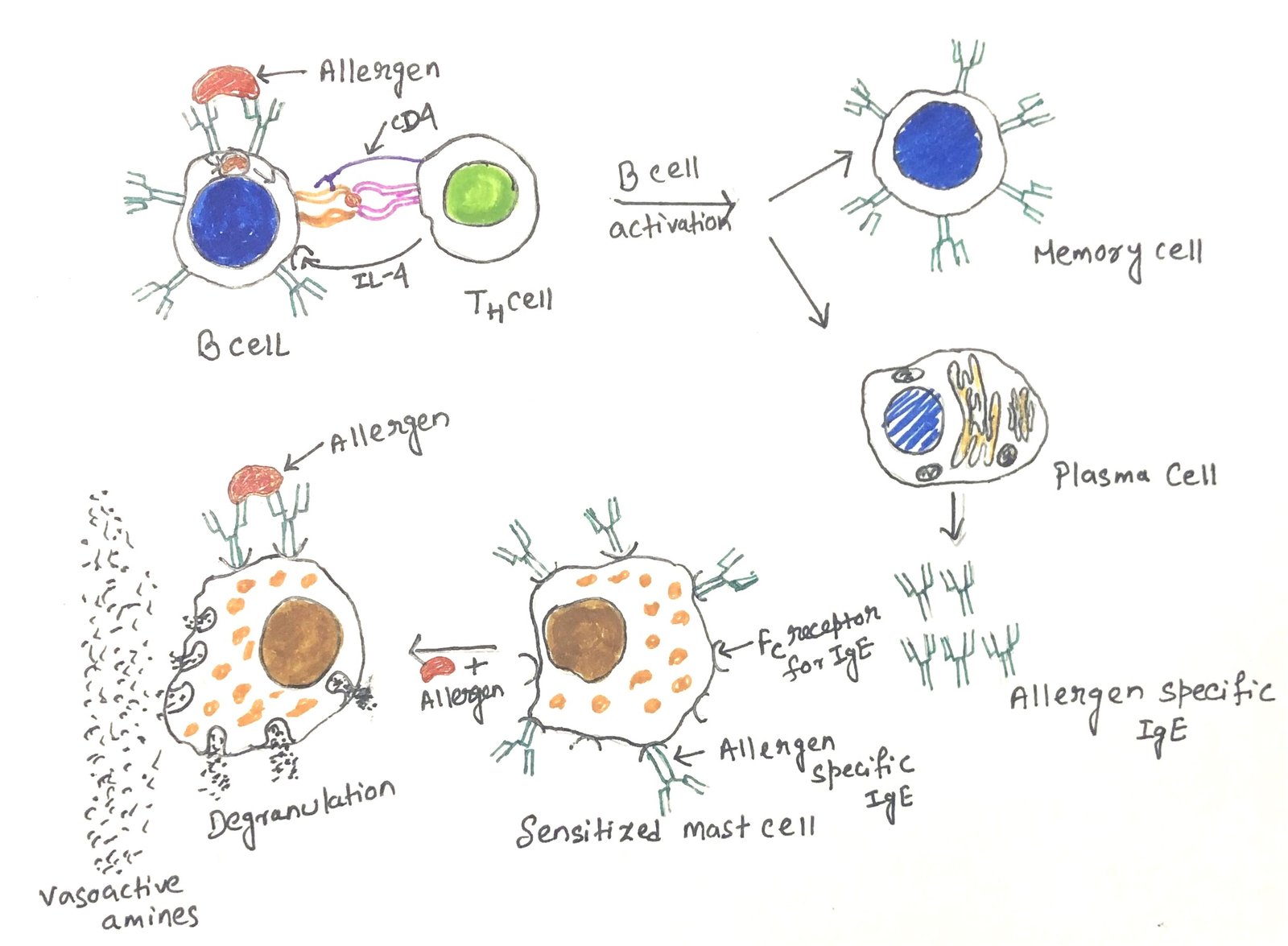
Plasma cells produce IgE antibodies in response to stimulation of TH2 cells by an antigen. The IgE antibodies mediate type I hypersensitivity. This class of antibody binds with high affinity to Fc receptors on the surface of tissue mast cells and blood basophils. The IgE-coated mast cells and basophils become sensitized, and a second exposure to the same allergen cross-links the membrane-bound IgE on the sensitized mast cells and basophils. This results in the degranulation of these cells.
Atopic Disorders
An exaggerated IgE-mediated immune response is known as atopy. All atopic disorders belong to type I hypersensitive reactions. Atopy is a hereditary predisposition to the development of immediate hypersensitivity reactions against common environmental antigens. Atopic individuals have defects in IgE antibody regulation, thus allowing non-parasitic antigens to spur inappropriate IgE production, which leads to the development of type-I hypersensitivity. These individuals are more susceptible to allergies such as hay fever, eczema, and asthma. Atopic disorders most commonly affect the nose, eyes, skin, and lungs.
Allergic Disorders
An allergy is an exaggerated immune response to a foreign antigen, regardless of the mechanism. The non-parasitic antigens, also called allergens, are capable of stimulating type-I hypersensitive responses in allergic individuals. An allergen induces type I IgE-mediated or type IV T-cell–mediated immune responses. The allergens that enter the body by either inhalation or ingestion elicit the IgE responses on the surface of mucous membranes. Common allergens associated with type-I hypersensitivity are proteins, plant pollens, drugs, foods, insect products, or mold spores.
Some allergens have been purified and characterized. These allergens are extracted from rye grass pollen, ragweed pollen, codfish, birch pollen, timothy grass pollen, and bee venom. Most allergens are small proteins or protein-bound substances having a molecular weight between 15,000 and 40,000 and appear to possess diverse properties. Some allergens are potent antigens (foreign serum and egg albumin), whereas others are weak antigens (plant pollens).
Degranulation of Mast Cells and Blood Basophils
Allergen cross-linkage of bound IgE generally initiates the degranulation of mast cells and basophils. Other stimuli, such as the anaphylatoxins, such as C3a, C4a, and C5a, various drugs, exercise, emotional stress, and some chemicals, can also start the process of degranulation. These reactions, without IgE-allergen interaction, though, produce the same symptoms as hypersensitivity but are not called hypersensitive reactions.
When we are exposed to an allergen, B cells get activated to form IgE-secreting plasma cells. The secreted IgE molecules bind to IgE-specific Fc receptors on blood basophils and mast cells. The IgE-coated mast cells and basophils then become sensitized. When a second exposure to an allergen occurs, the IgE-mediated degranulation begins by cross-linking the IgE that is bound to the Fc receptor on the surface of a mast cell or blood basophils (Figure 1).

This leads to the release of pharmacologically active mediators and vasoactive amines from mast cells and basophils. Just after cross-linkage, methylation of various membrane phospholipids takes place. This methylation causes an increase in membrane fluidity and the formation of Ca2+ channels. The increase of Ca2+ is a necessity in degranulation. The drug sodium cromoglycate blocks the influx of Ca2+ as a treatment for allergies.
Along with phospholipid methylation and an increase in Ca2+, there is a transient increase in the activity of membrane-bound adenylate cyclase, with a brisk peak of its reaction product, cAMP (cyclic adenosine monophosphate). The increase in cAMP is short-term, which is followed by a drop in cAMP levels. This drop in the level of cAMP aids in the process of degranulation. The drugs for the treatment of allergies increase the cAMP levels.
The Mediators Mediating Type-I Reactions
Many mediators, like pharmacologically active agents, mediate type I reactions. These mediators act on local tissues and also on secondary effector cells, such as eosinophils, neutrophils, T lymphocytes, monocytes, and platelets. The mediators are of two types, i.e., primary mediators and secondary mediators.
The primary mediators are produced before degranulation and are stored in the granules. Histamine, proteases, eosinophil, chemotactic factor, neutrophil chemotactic factor, and heparin are the significant primary mediators. The secondary mediators include platelet-activating factors, leukotrienes, prostaglandins, bradykinins, and various cytokines. The membrane phospholipids release secondary mediators during the degranulation process. The secondary mediators are also synthesized after target cell activation. These mediators mainly help in smooth muscle contraction and vasodilation.
The platelet activation factor amplifies the reaction and causes platelet aggregation, which leads to the release of histamine, heparin, and vasoactive amines. After release from mast cells, histamine initially binds to specific receptors, i.e., H1, H2, and H3, on various target cells. Most of the biological effects of histamine in allergic reactions are mediated by the binding of histamine to H1 receptors. This binding brings many changes, such as the contraction of intestinal and bronchial smooth muscles, increases the permeability of venules, and increases mucus secretion by goblet cells.
Histamine interacts with H2 receptors, thus increasing vascular permeability and dilation. It stimulates exocrine glands. Histamine binds to H2 receptors on mast cells and basophils, leading to suppression of degranulation, therefore exerting negative feedback on the release of mediators. The effects of leukotrienes and prostaglandins are more pronounced and longer-lasting than those of histamine. Mast cells secrete cytokines (IL-4, IL-5, IL-6, and TNF-α) that alter the local microenvironment, eventually leading to the recruitment of inflammatory cells such as neutrophils and eosinophils.
Type-I Reactions: Clinical Manifestations
Systemic Anaphylaxis
Anaphylaxis is a severe form of allergic response, which is systemic and fatal and occurs within minutes of exposure to an allergen. It is usually initiated by an allergen introduced directly into the bloodstream or absorbed into the circulation from the gut or skin. The symptoms appear in the form of a lowering in blood pressure, leading to anaphylactic shock. The shock is followed by smooth muscle contraction, leading to defecation, urination, and bronchiolar constriction. This eventually leads to asphyxiation, which can cause death within 2-4 minutes of exposure to the allergen. The agile and widespread IgE antibody-mediated degranulation of mast cells and basophils, and the systemic effects of their contents, are responsible for the development of fatal symptoms.
In susceptible humans, systemic anaphylaxis is triggered by a wide range of antigens, which include the venom from bees, wasps, hornet ants, drugs like penicillin, insulin, and antitoxins, seafood, and nuts. It is a fatal state whose onset occurs within minutes of a type-I hypersensitive reaction. Epinephrine, the drug for systemic anaphylactic reactions, thwarts the effects of mediators like histamines and leukotrienes by relaxing the smooth muscles and reducing vascular permeability. Epinephrine blocks degranulation by increasing cAMP levels in the mast cell.
Localized Hypersensitivity
Localized hypersensitivity reactions include atopic allergies such as allergic rhinitis (hay fever), asthma, atopic dermatitis (eczema), and food allergies. The reaction is limited to a specific target tissue or organ.
Asthma
It is a common chronic inflammatory disease of the airways. Asthma is triggered by airborne or blood-borne allergens or viral antigens (atopic) or may be induced by exercise or cold, independent of allergen stimulation (non-atopic). The symptoms of an asthmatic attack are shortness of breath, wheezing, and chest tightness.
Asthma is triggered by the degranulation of mast cells with the release of mediators in the lower respiratory tract. The resulting contraction of the bronchial smooth muscles leads to bronchoconstriction. Asthmatic patients have increased expression of receptors for a peptide P, which contracts bronchial smooth muscles, and have decreased expression of receptors for vasoactive intestinal peptide, which relaxes smooth muscles.
Early and late-phase response in Asthma
Type-I hypersensitivity responses have an immediate early response and one or more late-phase responses. The disease Asthma includes an early response, which occurs within minutes of allergen exposure. This leads to the release of mediators, such as histamine, leukotrienes(LTC4), and prostaglandin (PGD2), causing bronchoconstriction, vasodilation, and some buildup of mucus.
Hours after the immediate phase of a type-I hypersensitive reaction begins to subside, the late-phase reaction begins. It involves additional mediators, including IL-4, IL-5, IL-16, TNF-α, eosinophil chemotactic factor(ECF), and platelet-activating factor(PAF). These mediators increase endothelial cell adhesion and cause an influx of inflammatory cells, including eosinophils and neutrophils into the bronchial tissue. The neutrophils and eosinophils release toxic enzymes, oxygen radicals, and cytokines, which lead to the obstruction of the bronchial lumen with mucus, proteins, and cellular debris. This eventually leads to the discarding of the epithelium, thickening of the basement membrane, building up of fluid, and hypertrophy of the bronchial smooth muscles. A mucus plug often forms and attaches to the bronchial wall. The plug contains clusters of detached epithelial-cell fragments, eosinophils, some neutrophils, and spirals of bronchial tissue known as Curschmann’s spirals (Figure 2).

Quick-relief medications are used to treat acute symptoms of asthma, whereas long-term medications are used to prevent further exacerbation.
Allergic Rhinitis
Hay fever or allergic rhinitis is the most common localized hypersensitive reaction. Inhaling common airborne allergens ( pollens, dust, mold spores) causes the symptoms to appear. These allergens are recognized by IgE antibodies bound to sensitized mast cells in the conjunctival and nasal mucosa. The receptor-bound IgE crosslinks the allergen and induces the release of histamine and other mediators from tissue mast cells. The release of histamines and mediators results in vasodilation, an increase in capillary permeability, and the production of secretions in the eyes, nasal passages, and respiratory tract. The symptoms appear in the form of tears, a runny nose, sneezing, and coughing. Allergic asthma is triggered in the same way as hay fever, i.e., by the activation and degranulation of mast cells with subsequent release of inflammatory mediators. However, instead of occurring in the nasal mucosa, the reaction occurs deep in the lower respiratory tract.
Allergic conjunctivitis is an eye inflammation. It is initiated by IgE-activated mast cell mediators, which are caused by airborne allergens such as pollen. The early phase symptoms include itching, redness, tearing, and edema, which can continue further and develop into eosinophilia and inflammation.
Allergic Eczema
It is also known as atopic dermatitis, which is an allergic skin inflammatory disease. It is seen mostly in young children. The disease is marked by elevated levels of serum IgE. An individual suffering from this disease usually develops a rash and skin eruptions filled with pus in case of bacterial infection. Skin delayed-type hypersensitivity often involves TH17 or TH1 cells, whereas the skin lesions in atopic dermatitis contain TH2 cells with an increased number of eosinophils.
Some common triggers of allergic eczema are nickel(found in earrings, jewelry, belt buckles, and metal buttons on jeans), perfumes found in cosmetics, certain clothing dyes, hairdressing chemicals and hair dye, latex, adhesives, antibiotic creams or ointments, etc. Allergic eczema may also result when the skin is exposed to chemicals in the presence of sunlight.
When the skin releases histamine, it induces leakage of small blood vessels, producing localized areas of redness and swelling. This is known as atopic urticaria or hives.
Food Allergies
Many foods can trigger anaphylaxis in allergic individuals, whose incidence is on the rise. In children, food allergies are the major anaphylactic response when compared to others. This is because of the transport of food allergens across the gut wall and into the circulation. The most common food allergies for children are found in cow’s milk, eggs, peanuts, tree nuts, soy, wheat, fish, and shellfish.
Most of the food allergens are water-soluble glycoproteins that show stability to heat, acid, and proteases. This makes them undergo slow digestion. The cross-linking of allergen with IgE on mast cells along the upper or lower gastrointestinal tract can induce localized smooth muscle contraction and vasodilation. It leads to the appearance of symptoms such as itching with rashes, nausea, abdominal pain, vomiting, and diarrhea. The signs and symptoms may range from mild to severe and can develop within minutes to 2 hours of allergen ingestion.
Some individuals may have oral hypersensitivity and experience symptoms like tingling of the lips, palate, and throat. The permeability of mucous membranes increases by the degranulation of mast cells along the gut. As a result, the allergen enters the bloodstream. Various symptoms can develop depending on the position of the allergen.
Some people develop asthmatic attacks after ingesting certain foods, while others develop atopic urticaria, commonly known as hives (when a food allergen is carried to sensitized mast cells in the skin). Sometimes, food allergies may be directly caused by cells instead of IgE-induced mediators from mast cells and basophils. Allergens can directly activate granulocytes to degranulate. They can also activate the product of T cells, which may contribute to local responses.
Conclusion
Type I hypersensitive reaction is an allergic reaction that is induced by certain types of antigens known as allergens. The IgE antibodies mediate type I hypersensitivity. All atopic disorders belong to type I hypersensitive reactions. An allergy is an exaggerated immune response to a foreign antigen, regardless of the mechanism. Common allergens associated with type-I hypersensitivity are proteins, plant pollens, drugs, foods, insect products, or mold spores. Allergen cross-linkage of bound IgE generally initiates the degranulation of mast cells and basophils.
There are two types of mediators mediating type-I hypersensitive reactions. Histamine, proteases, eosinophil, chemotactic factor, neutrophil chemotactic factor, and heparin are the significant primary mediators. The secondary mediators include platelet-activating factors, leukotrienes, prostaglandins, bradykinins, and various cytokines.
The clinical manifestations of type-I hypersensitivity include systemic anaphylaxis and localized hypersensitivity. Systemic anaphylaxis is a severe form of allergic response, which is systemic and fatal and occurs within minutes of exposure to an allergen. In susceptible humans, systemic anaphylaxis is triggered by a wide range of antigens, which include the venom from bees, wasps, hornet ants, drugs like penicillin, insulin, and antitoxins, seafood, and nuts. Localized hypersensitivity reactions are limited to a specific target tissue or organ. They include atopic allergies such as allergic rhinitis (hay fever), asthma, atopic dermatitis (eczema), and food allergies.
You may also like:

I, Swagatika Sahu (author of this website), have done my master’s in Biotechnology. I have around fourteen years of experience in writing and believe that writing is a great way to share knowledge. I hope the articles on the website will help users in enhancing their intellect in Biotechnology.