
In this article, I briefly describe the basics of organ transplantation.
Organ Transplantation
Removing an organ from one’s body and placing it in a recipient’s body to fulfill the need for a missing organ is known as organ transplantation. In the fifth century B.C., the legendary surgeon from India, Sushruta, expressed nose reconstruction for the first time. This process required the collection and transfer of skin from one site to another. Today, this type of transfer is known as an autograft and is most likely to succeed.
Joseph Murray and colleagues in Boston, in the year 1954, first successfully transplanted a kidney between identical twins. However, tackling the obstacle of MHC molecules took nearly seven years. Dr. Samuel Kountz, an African American transplant surgeon at Stanford, along with a team of surgeons, completed the first non-twin living human transplant. In this procedure, a kidney from a mother is transplanted to her daughter. This pioneering work with immunosuppressants and a new kidney perfusion technique emerged as a new hope among physicians for the success of organ transplantation worldwide. Today, the transfer of various organs between non-identical individuals is being done with more frequency and a high success rate. However, the immediate availability of organs still becomes a scourge for the patients and the physicians as well.
Over 30,000 solid organ transplants were performed in the US in the year 2016. Though the clinical outcomes have progressed considerably, the process is facing major obstacles. Immunosuppressive drugs play a vital role in increasing the short-term survival of the transplant. However, they cause medical complications in patients. New research with new treatments that promise more specific tolerance to the transferred tissue without any hindrance to immune function is under development.
The Low Supply of Organs
Transplantation is the only method of treatment for many medical conditions. Organ failure may be a cause of birth defects, infection, burns, trauma, or chronic disease that can be corrected through tissue or organ transplantation. The demand for donor tissue increases every year, which continuously decreases the supply. According to a survey by The American Transplant Foundation, every day, nearly twenty people succumb to their medical conditions while waiting for organ transplantation. Many patients also do not survive the years-long wait due to the short supply of available organs.
Different Types of Transplants
There are different types of tissue transplants, and the type of immune response to a transplant varies with the type and source of the grafted tissue. Generally, four types of transplants are done, i.e., autograft, isograft, allograft, and xenograft.
- Autograft: It involves the transfer of self-tissue from one body site to another in the same individual.
- Isograft: It involves the transfer of tissue between genetically identical individuals, e.g., in identical twins. It can be done in an inbred strain of mice, with a syngenic donor and recipient.
- Allograft: It involves the transfer of tissue between genetically different members of the same species. It is the most common tissue graft done between non-identical humans or different strains of mice.
- Xenograft: It is the process where tissue transfer is done between different species.
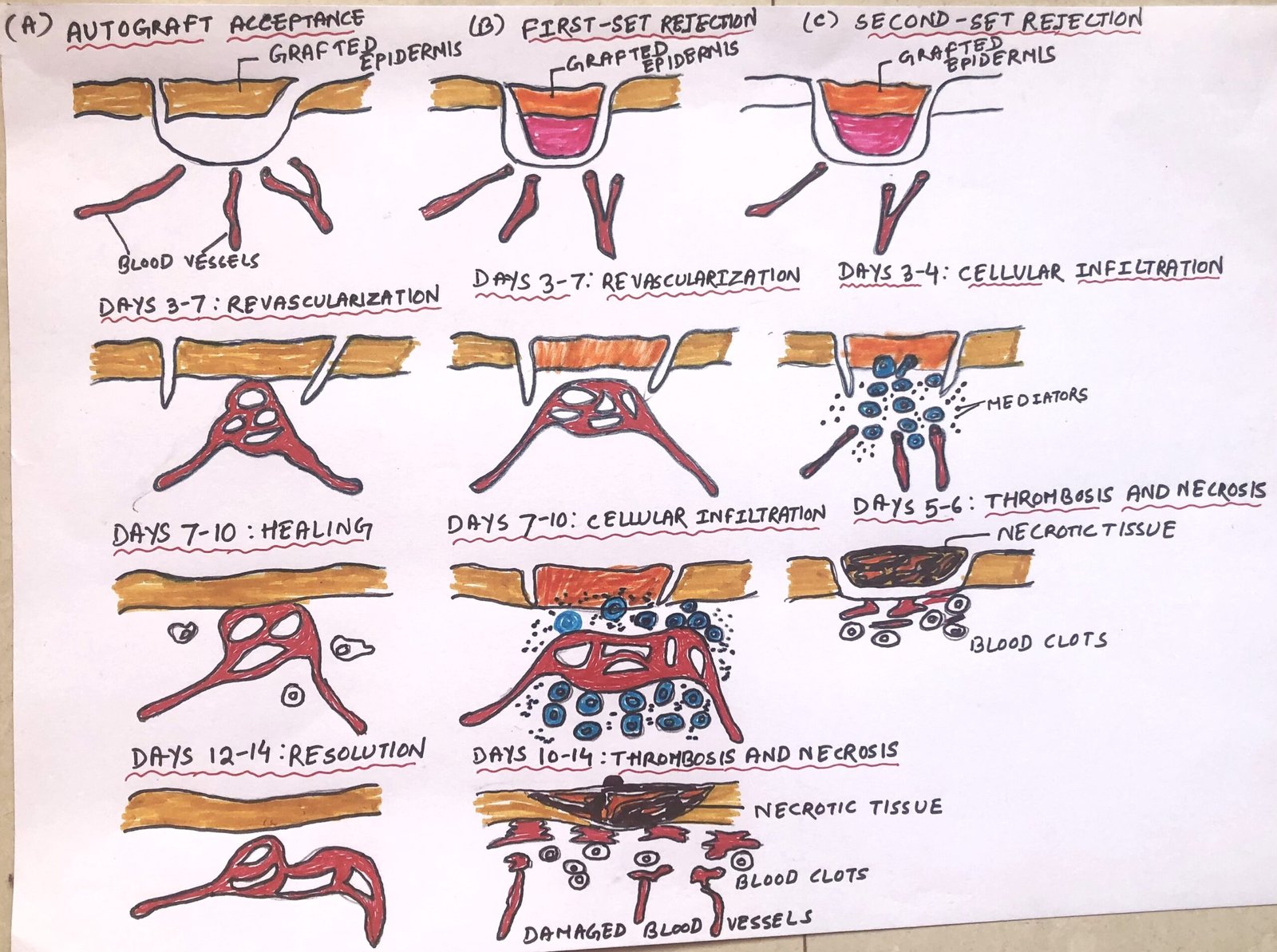
Autografts and isografts pertain to the genetic identity between donor and recipient. So, they are usually accepted (Figure 1-A). If the tissues share much antigenic similarity, then the transfer happens without immunologic rejection. The tissues are said to be histocompatible. This involves the transfer between identical twins or between members of the same mouse strain.

Allografts
In allografts, tissue transfer is done between genetically different members of the same species. Thus, tissues display marked antigenic disparity and are said to be histo-incompatible, inducing an immune response leading to tissue rejection. The antigens involved in the process of transplantation are encoded by more than forty different loci. However, the loci responsible for the most frequent allograft rejection are located within the major histocompatibility complex (MHC). The genes in the MHC locus are closely linked and are usually inherited as a complete set from each parent, known as a haplotype. So, xenografts between different species suffer the most genetic and antigenic disparity, leading to a quick and strong graft rejection response.
Allograft Rejection
The rejection rate of allografts differs depending on the type of tissue involved. Generally, the rate of rejection of skin grafts is more compared to other tissues, e.g., kidney, heart, etc. However, the immune response in graft rejection shows the features of immune specificity and memory.
It can be understood by taking an example of an inbred mouse of strain A and grafting it with skin from strain B. Then, the first set of rejections occurs, which is also called primary graft rejection (Figure 1-B). The skin first gets revascularised within three to seven days. Then, with the development of the reaction, the vascularized transplant becomes infiltrated with inflammatory cells. There is a reduction in vascularization of the transplanted tissue within seven to ten days. After ten days, tissue necrosis is visible. The complete rejection of the graft is observed after 12-14 days. It is an example of a primary response to non-self antigens.
When a second strain-B graft is transferred to a formerly engrafted strain-A mouse, it induces a secondary response, and immunologic memory is noticed. In this grafting procedure, the anti-graft reaction develops more quickly, with complete rejection of the graft occurring within five to six days. This is called second-set rejection (figure 1-C), which happens mainly because of the recall of graft-specific T and B cells.
Disparity among Organs in Transplantation
The organs in our body do not show the same response to transplantation. Some organs show more positive responses than others. Kidney transplantation is the most successful among all organ transplants to date. The first kidney transplant was done in the 1950s, and till now nearly 500,000 kidneys have been transplanted worldwide.
The liver is the second most frequently transplanted organ after the kidney, which is followed by the transplantation of the heart, lung, and pancreas. Lack of oxygen causes tissue damage, which is a major limitation in the transplantation process. Before the transplantation of the organ, cell death causes the release of damage-associated molecular patterns (DAMPs), leading to the development of a proinflammatory microenvironment. The damage and inflammation can be brought down by shortening the time spent of an organ outside the body and by improving the preservation techniques at that time. This can lower the rejection rate and enhance graft survival.
Factors Linked to Organ Transplantation and Cell Transplantation
Before a transplantation procedure, many factors are taken into consideration, e.g., alternative treatment options, availability of organs, and the level of difficulty of the procedure. Many diseases lead to the dysfunction of organs, e.g., diabetes is responsible for kidney failure, and a patient has to be on dialysis till the availability of a suitable organ. Kidney is available from living as well as deceased donors. A patient can survive only with a single kidney, though they come in pairs. Kidneys can survive for a longer time outside the body when compared to any other organ.
Patients suffering from hematologic diseases like leukemia, lymphoma, and inherited immune deficiencies, like severe combined immunodeficiency (SCID), need transplantation of cells rather than a solid organ. Transplanting cells involves the transfer of bone marrow or hematopoietic stem cells to patients.
The avilability of bone marrow or hematopoietic stem cells is easier when compared to solid organs as the former is a renewing resource. However, getting a matched donor is a solid obstacle in cell transplantation. The donor and recipient must share MHC alleles, with some loci than others. Donors with only a partial HLA match can be quickly identified by tissue-typing techniques. However, very few individuals are registered in the bone marrow section, and it’s arduous to find some alleles among ethnic minorities.
Before a bone marrow transfer, the individuals are made highly immunosuppressed, which minimizes the graft rejection when a match is available. However, the graft-versus-host-disease (GvHD) becomes a challenge as the introduction of immunocompetent cells from a foreign donor causes the transplant to attack host alloantigens, or foreign MHC molecules present on recipient tissues. Nowadays, the occurrence of GvHD is reduced by depleting T cells before transfer. But still, this remains an obstacle to the success of bone marrow transplants.
Heart Transplantation
Heart and lung transplantation involve some crucial steps to make it successful. In this process, the recipient must be kept alive artificially during the time of surgery. The human heart can remain viable for a few hours and is kept in ice-cold buffer solutions, which delay the damage process. Present-day technological advancement suggests keeping the heart warm and oxygenated for transport, which is also called ”heart in a box”. However, the lack of oxygen and the deprivation of ATP can lead to irreversible organ damage.
The first heart transplantation was carried out by Dr. Christian Barnard in 1964 in South Africa. Presently, the survival rate of heart transplant patients has increased to more than 80%. The source of this transplantation is typically brain-dead individuals with an intact circulatory system and functioning heart. Because of the limited supply of organs and the urgency of transplant, HLA matching between donor and recipient is not always possible. However, MHC matching is possible if the heart can survive outside the body for longer periods.
Liver transplantation
The liver is the largest essential organ of the body that performs many vital functions. It filters all of the blood in the body and plays an important role in breaking down poisonous substances. The liver regulates blood sugar levels and creates essential nutrients. It produces bile, which helps digest fats and carry away waste. The liver can not function properly due to viral diseases, liver cancers, and exposure to harmful chemicals. Most liver transplants are done to correct congenital abnormalities. The liver possesses intricacy in its circulatory network, thus posing some challenges during the transplantation process. The large size of the liver has an advantage, as from a single donor it can be split and given to two or more recipients.
The disease type 1 diabetes is caused by the improper functioning of the insulin-producing islet cells in the pancreas. According to the new protocol, instead of transferring the whole organ, donor islet cells are harvested and transferred into the recipient’s liver. These cells are then permanently established in the liver sinusoids. After the transplantation, the results show that more than half of the recipients do not show dependency on insulin.
Skin Transplantation
Skin transplants generally involve autografts, which include the transfer of healthy tissue from one site to another in the same individual. However, patients suffering severe burns require the transfer of foreign skin. But fresh tissue is not always available, and frozen grafts can be used as a replacement. Sir Peter Medawar first made use of frozen skin samples to treat burn victims in the Second World War. He was conferred with the Nobel Prize in 1960 for his work on immune tolerance. These thawed skin grafts are unable to proliferate, thus act as biologic dressings. They can promote healing and protect the delicate tissues underneath. Researchers from Brazil are currently evolving the use of sterilized tilapia fish skin, which has been shown to protect underlying tissue and reduce the time of healing wounds in persons with severe burns.
Conclusion
Organ transplantation is the process of removing an organ from an individual and placing it in a recipient’s body in place of a non-functioning organ. Dr. Samuel Kountz, an African American transplant surgeon at Stanford, along with a team of surgeons, completed the first nontwin living human transplant. This process involves the transfer of a kidney from a mother to her daughter. Today, the transfer of various organs between non-identical individuals is being done with more frequency and a high success rate. However, organ availability remains a major problem.
Generally, four types of transplants are done, i.e., autograft, isograft, allograft, and xenograft. The process of transplantation varies among organs, as kidney transplantation is the most frequently done compared to other organs. The liver is the second most frequently transplanted organ after the kidney, which is followed by the transplantation of the heart, lung, and pancreas.
Patients suffering from hematologic diseases like leukemia and lymphoma, and inherited immune deficiencies, like severe combined immunodeficiency (SCID), need transplantation of cells rather than a solid organ. Transplanting cells involves the transfer of bone marrow or hematopoietic stem cells to patients.
The source of heart transplantation is typically brain-dead individuals with an intact circulatory system and functioning heart. The liver possesses a complicated circulatory network, thus posing some challenges during the transplantation process. Skin transplants generally include autografts. However, patients suffering severe burns need foreign skin, and in this case, frozen grafts are used as a replacement.
With the progress of time, transplantation success with more developed procedures for inducing tolerance, controlling rejection, and expanding sources for transplanted tissue would only increase.
You may also like:
- Expression of MHC molecules
- Pre-Transplantation Tests for Organ Transplantation
- The Immunology Behind Graft Rejection
- Therapeutic Approaches to Immune Suppression

I, Swagatika Sahu (author of this website), have done my master’s in Biotechnology. I have around fourteen years of experience in writing and believe that writing is a great way to share knowledge. I hope the articles on the website will help users in enhancing their intellect in Biotechnology.